nl
nl
 Nederlands
Nederlands

Surgery for lung cancer / thorax
A team of specialists at the Netherlands Cancer Institute will support you through your surgery. This team consists of medical specialists, [physician assistants and clinical nurse specialists. Our (thoracic) surgeons closely collaborate with our pulmonologists (lung specialists) during your surgery, while our anesthesiologists handle your anesthesia and pain treatment. Our physical therapist can help you prepare for the surgery and support your recovery.
Knowing you have to have thoracic surgery can be stressful and uncertain. To support you and your lived ones through this period, our clinical nurse specialists will be your direct contact point during the entire process.
Meet our NKI Lung Cancer Center team, or read more about the different types of thoracic surgeries available at the Netherlands Cancer Institute as well as our care.
We have combined all our information about the lungs and thorax on this page, as the two are anatomically related.
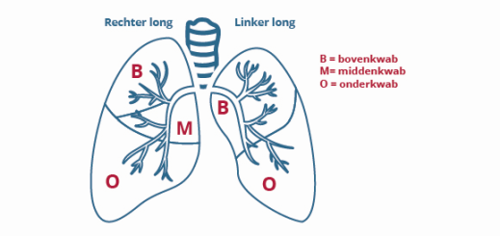
The lungs - position, structure, and function
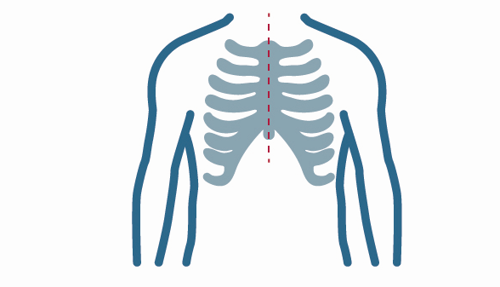
The right and left lung are found in the chest (thorax) on both sides of the heart. The right lung has three lung lobes, while the left lung has two. Every lung is covered by a membrane, the pleura. The area between the lungs is called the mediastinum. This is where you will find the heart, trachea (part of the airways), esophagus, blood vessels, nerves, lymph nodes and lymphatic vessels.
The air you breathe in through your nose or mouth reaches the lungs through your oral cavity. The airways lead to two large branches that lead to the lungs, where they branch out even further into the small vesicles. The lungs take in oxygen.
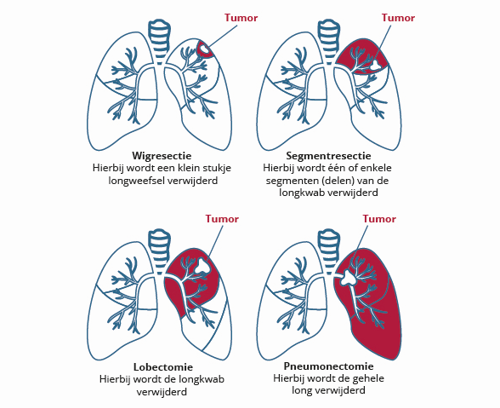
Types of procedures
Below are images of two types of procedures. We expand more on them on this page.
What is a pneumonectomy?
A pneumonectomy is a surgical procedure to remove a lung - either the right side, or the left. This is a major surgery that can only be done if the other lung functions well. This procedure is usually done through the classic approach (thoracotomy).
What is a lobectomy?
The left lung has two loves, and the right lung has three. A lobectomy is a surgical removal of the lung lobe which has a tumor. The lymph nodes next to the tumor will be removed as well. We can use an open surgery technique (thoracotomy) or laparoscopic surgery (VATS) or robot-assisted surgery (RATS).
What is a segment resection?
The lung lobes consist of various segments. A segment resection is a surgical procedure to remove one or more of these segments. This procedure can remove certain tumor types in the lung. This type of surgery will usually be laparoscopic (VATS).
What is a wedge resection?
A wedge resection is a surgical procedure that remives a part of the lung lobe in the shape of a wedge (a pizza slice). This surgery aims to remove metastases in the lungs. The tissue will be send to a pathologist for analysis. This surgery can be open surgery (thoracotomy), but is usually laparoscopic (VATS).
Surgery for mesothelioma, asbestos cancer
Under very specific circumstances patients with mesothelioma can have surgery. Surgery for mesothelioma is not always beneficial. Surgery is only done as part of a trial, for a small number of patients.
Surgery for tumors behind the sternum (mediastinum) like thymoma
if you have an abnormality behind the sternum, like a thymoma (a tumor of the thymus), you may need surgery to remove it. We can remove it with a RATS or sternotomy procedure. Depending on the exact abnormality and its location, your surgeon will decide which option is best for you.
Surgery techniques
What is a VATS?
VATS stands for Video Assisted Thoracic (or Thoracoscopic) Surgery. It is a surgery of the thorax (chest) using a surgical camera and video monitor. The VATS is a keyhole, or laparoscopic surgery, also known as a thoracoscopic procedure.
We use a thoracoscope for laparoscopic surgeries: a time with a small camera and light attached to the end. The thoracoscope is connected to a TV monitor allowing the surgeon to see the surgery.
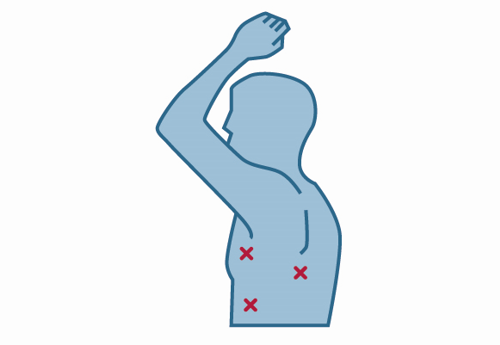
Your surgeon will make 2 to 4 small incisions in the skin between the ribs. See the image below for the exact placement. To allow for sufficient space, the anesthesiologist will collapse the lung requiring surgery by halting your breathing to that lung while you will receive your oxygen through the other lung. Your surgeon will insert 2 or 3 tubes into the thorax through the incisions. The surgeon can see the inside of your body on the screen connected to the camera, so a large incision won’t be necessary. Your surgeon can then remove the tissue using instruments inserted through the other tubes. Smaller tumors or entire lung tubes can be removed using special staplers. After the procedure, the incisions will be stitched back together and your lung will receive oxygen again, reinflating them to their usual shape.
Not all tumors can be removed through VATS. If your tumor attached itself to the lung tissue, or if you have received radiation therapy in the past, or if we cannot properly see the abnormality or if we encounter unforeseen complications of bleeding during surgery. During the surgery, we may find out that your situation is more complex than we had initially thought. Your surgeon may need to make a bigger incision (thoracotomy) to properly treat you.
What is a RATS?
RATS stands for Robot Assisted Thoracic (of Thoracoscopic) Surgery. We use a RATS to remove tumors in the lungs and behind the sternum. A RATS is a laparoscopic (keyhole) surgery, just like a VATS. The only difference is that all operations are done by a robot controlled by your thoracic surgeon, who is seated in a ”cockpit”. The robot gives the surgeon an enlarged and 3D image of the area which allows for great precision. Because the robot is beneficial in certain kinds of surgeries compared to the VATS, the robot is only used if this procedure has an advantage. Recovery time after RATS is usually quicker than after open surgery (thoracotomy or sternotomy).
What is a thoracotomy?
A thoracotomy is a surgical procedure which opens the chest to access the chest cavity or lungs. Your surgeon will make an incision between the ribs (on the left or right side). The exact location will depend on the location of your abnormality.
What is a sternotomy?
A sternotomy is a surgical procedure in which your sternum is opened vertically. After making an incision in the skin, your surgeon will saw through the bone of the sternum. This allows your surgeon access to the chest to remove the abnormality. The sternum will be sewn back together using steel wire, allowing it to close. These wires won’t need to be removed and can remain in place indefinitely.